Jesse Smedley
Jesse Smedley is the Principal Broker for iHealthBrokers and the founder, president, and CEO of Smedley Insurance Group, Inc. and iHealthBrokers.com. Since the inception of SIG in 2007, Jesse has been dedicated to helping people save money on their health insurance by providing them with resources to educate themselves on all their health insurance options, both under age 65 and Medicare beneficiaries. He is featured in many publications as well as writes regularly for expert columns regarding health insurance and Medicare.
The Face of Future Health Care
March 20, 2013
By REED ABELSON
OAKLAND, Calif. — When people talk about the future of health care, Kaiser Permanente is often the model they have in mind.
The organization, which combines a nonprofit insurance plan with its own hospitals and clinics, is the kind of holistic health system that President Obama’s health care law encourages.
Kaiser has sophisticated electronic records and computer systems that — after 10 years and $30 billion in technology spending — have led to better-coordinated patient care, another goal of the president. And because the plan is paid a fixed amount for medical care per member, there is a strong financial incentive to keep people healthy and out of the hospital, the same goal of the hundreds of accountable care organizations now being created.
“Over the course of the last 15 years, they’ve been just going into high gear and doing everything right,” said Dr. Thomas S. Bodenheimer, a health policy expert at the University of California, San Francisco who recently chose Kaiser as his own health plan.
Yet even with all of its effort, its chairman and chief executive, George C. Halvorson, acknowledges Kaiser has yet to achieve the holy grail of delivering that care at a low enough cost. He says he and other health systems must fundamentally rethink what they do or risk having cost controls imposed on them either by the government or by employers, who are absorbing the bulk of health insurance costs. “We think the future of health care is going to be rationing or re-engineering,” he said.
Mr. Halvorson is convinced that Kaiser’s improvements in the quality of care save money. But he also says that the way to get costs lower is to move care farther and farther from the hospital setting — and even out of doctors’ offices. Kaiser is experimenting with ways to provide care at home or over the Internet, without the need for a physical office visit at all. He also argues that lower costs are going to be about finding ways to get people to take more responsibility for their health — for losing weight, for example, or bringing their blood pressure down.
“The obesity work is incredibly difficult,” he said. “It’s very, very hard to move the needle.”
Other health care experts say that while Kaiser has a place in the future, whether it is the best model for the country’s health care remains unclear. “They have not translated some of their strengths into better prices,” said David Lansky, the president and chief executive of the Pacific Business Group on Health, which represents employers on the West Coast, many of whom purchase coverage from Kaiser for their workers.
And there are other concerns, such as whether an all-encompassing system like Kaiser’s can really be replicated and whether the limits it places on where patients can seek care will be accepted by enough people to make a difference. Or whether, as the nation’s flirtation with health maintenance organizations, or H.M.O.’s, in the 1990s showed — people will balk at the concept of not being able to go to any doctor or hospital of their choice.
“The more you restrict the patient’s ability to do what they want, you risk reigniting the backlash we had in the past,” Mr. Lansky said.
In many ways, Kaiser has been ahead of the curve on health care for decades. Started by a surgeon running a tiny hospital near Desert Center, Calif., to serve construction workers, Kaiser became an H.M.O. with its own doctors and hospital in the mid-1940s and expanded beyond California over the next 50 years. But, as H.M.O.’s fell out of favor, it was forced to leave states like New York, Connecticut and Texas.
But Kaiser persevered, and its membership, which peaked in 1998, is now about the same as its previous high of 9.1 million, about three-quarters of whom are in California. It still operates in a half-dozen states from Maryland to Hawaii and is looking to expand in the Mid-Atlantic region, where membership had been dropping.
The organization, with some $50 billion in annual revenue, owns 37 hospitals and employs 17,000 doctors, all on salary. And its integrated model is in favor again. Hospitals across the country are buying physician practices or partnering with doctors and health insurers to form accountable care organizations, or A. C.O.’s, as a way of controlling more aspects of patient care. Doctors are also creating so-called medical homes, where patient care is better coordinated.
The days when doctors, hospitals and other providers are paid separately for each procedure will disappear eventually, health experts say. Instead, providers will have financial incentives to encourage them to keep people healthy, including lump sums to care for patients or provide comprehensive care for a specific condition. “All of care is going to move down this path, and it has to,” Mr. Halvorson said. “Medical homes are doing it; the very best A. C.O’s are going to figure out how to do it.”
The move by hospitals to buy physician practices is being viewed cautiously by health experts, who say there are downsides to the creation of large health care systems that may be motivated by the desire to increase their clout in the market, making it easier to fill beds and charge the insurers more for care. “They become these huge local monopolies,” said Dr. Robert Berenson, a health policy expert at the Urban Institute.
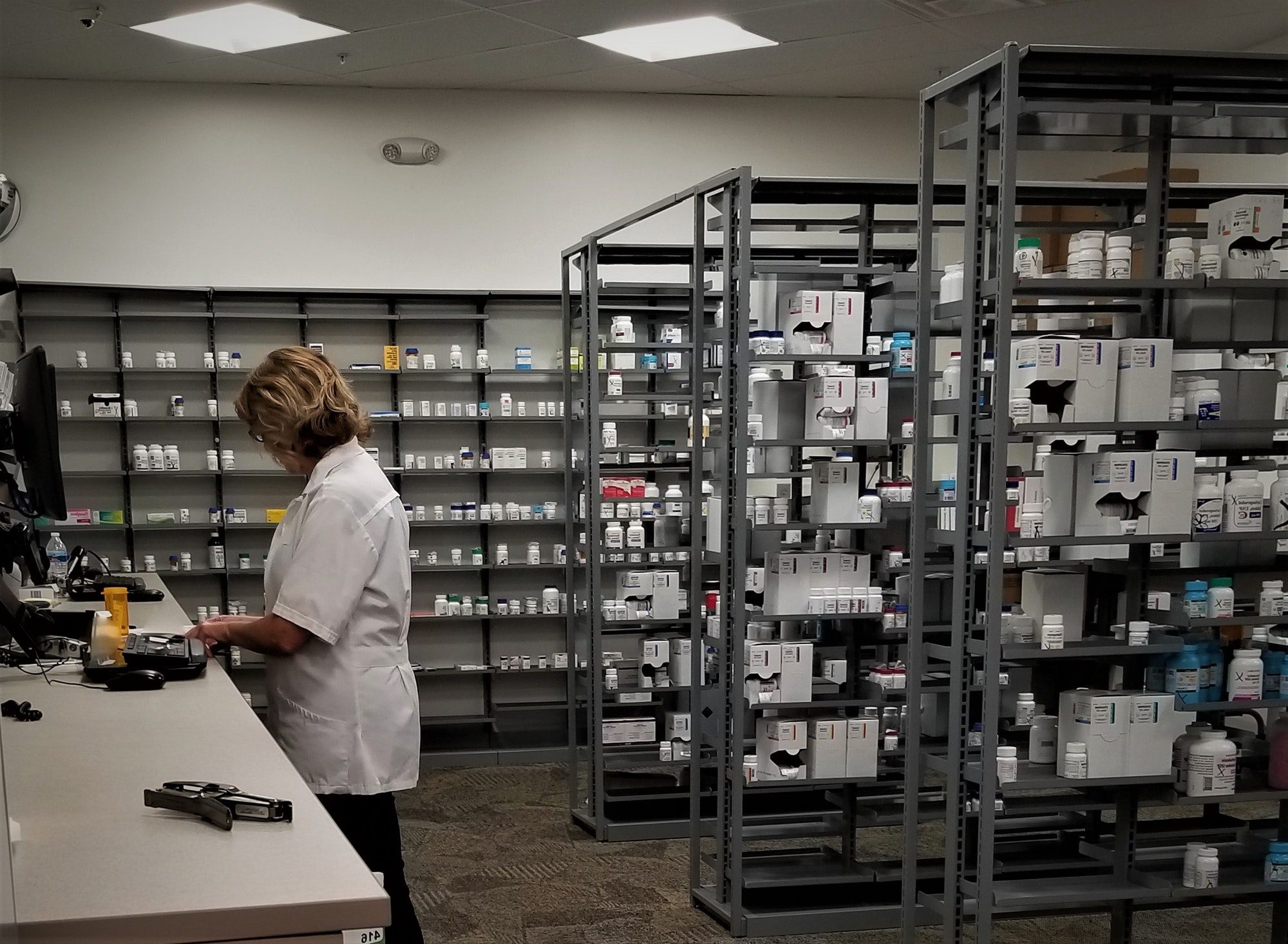
But having an integrated system seems essential to the success of Kaiser and a handful of similar, if smaller, organizations, like Intermountain Healthcare in Utah and Geisinger Health System in Pennsylvania, although some work with doctors whom they do not employ. In California, Kaiser controls nearly every aspect of a patient’s care, from providing the M.R.I. for a diagnosis to filling a prescription at one of its pharmacies to running a hospital where the patient undergoes surgery.
“We have all the pieces,” said Philip Fasano, Kaiser’s chief information officer. “Anything a patient needs you get in the four walls of our offices,” he said. As a result, while Kaiser can point to an analysis done by Aon Hewitt, a benefits consultant, showing that its plans are typically at least 10 percent less expensive than others, especially where they control all the providers, its costs are more like the average in places in Ohio, where it does not have its own hospitals and offer as broad a range of services.
And some patients outside of California, where Kaiser operations are less concentrated, complain about being forced to travel for treatment by Kaiser providers. Arva Priola, a 62-year-old Kaiser patient in Fredericksburg, Va., said her Kaiser doctors “are wonderful,” but that the plan recently started requiring her to get some treatments where they had physical facilities.
To get IV antibiotics after surgery, for example, she recently had to drive an hour and a half to a Kaiser office in Tysons Corner, Va. “Who wants to drive when you’re sick?” she asked. Kaiser says it is adding more services closer to Fredericksburg.
A California state agency recently criticized Kaiser for the long wait times its members had for mental health services and for providing inaccurate information about what services it provides. Kaiser says it has corrected the misinformation and is working to reduce and better track member wait times.
Where Kaiser has a head start that others may have difficulty catching up to is its use of electronic records and technology systems for tracking patient care.
When Dr. Jennifer Slovis, a Kaiser internist in Oakland, recently saw a patient, she was able to spot that the patient had an abnormal blood test several years ago. By reading through the patient’s medical history, she determined he was now overdue for an M.R.I. to check the status of a growth in his brain. She was able to e-mail his endocrinologist and schedule the necessary tests without the patient having to make an appointment with the specialist or her having to make her own diagnosis. “It saved a lot of starting over,” she said.
In the last five or so years, Kaiser has also been using the information to identify those doctors or clinics that excel in certain areas, as well as those in need of improvement. The organization has also used the records to change how it delivers care, identifying patients at risk for developing bed sores in the hospital and then sending electronic alerts every two hours to remind the nurses to turn the patients. The percentage of patients with serious pressure ulcers, or bed sores, dropped to well under 1 percent from 3.5 percent.
“The tool is an enabler to give information to people who give a damn,” said Dr. Jack Cochran, the executive who represents Kaiser’s physicians through the Permanente Federation.
Mr. Halvorson, the Kaiser chief, who plans to retire at the end of this year, says the organization is providing evidence to other health systems that re-engineering works. “All of that adds up to better care and cheaper care,” he said.